

Palavras-chave
má oclusão de Classe II
Como Citar
Resumo
Objetivo: Determinar a distribuição morfológica da má oclusão de Classe II de acordo ao padrão esquelético, em uma amostra da população adulta da Faculdade de Odontologia da Universidade do Chile.
Materiais e Métodos: A amostra experimental foi composta de 220 indivíduos acima de 18 anos de idade, com ângulo ANB maior que 4°. Os ângulos SNA e SNB foram medidos para determinar o padrão esquelético da Classe II.
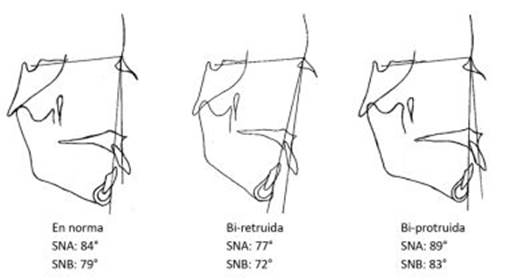
Resultados: Foi observado que o padrão esquelético mais frequente foi o mandibular e depois maxilar. Além disso, foram obtidos três novos tipos de padrões esqueléticos que, de acordo com a análise da literatura relevante, não haviam sido explicitamente descritos anteriormente: bi-protrusão, bi-retrusão e em norma.
Conclusões: O padrão esquelético mais frequente das más oclusões de Classe II do nosso estudo foi mandibular. As variantes bi-protrusão e bi-retrusão deveriam ser incorporadas no diagnóstico esquelético, especialmente a variante de bi-retrusão, devido à sua significativa frequência elevada e relevância clínica.
Referências
2. Narayanan RK, Jeseem M, Kumar TA. Prevalence of malocclusion among 10-12-year-old schoolchildren in Kozhikode District, Kerala: An epidemiological study. Int J Clin Pediatr Dent. 2016;9(1):50.
3. Angle EH. Classification of malocclusion. Dent Cosmos. 1899;41:350-75.
4. Massler M, Frankel JM. Prevalence of malocclusion in children aged 14 to 18 years. Am J Orthod 1951;37(10):751-68.
5. Rojas Valenzuela R, Carvajal R, Bustamante S, Silva AL, Rojas R. Estudio Cefalométrico de Harvold de los Tamaños Maxilares y de la Altura Facial Antero Inferior en Niños de 9 Años de Edad, con Clase I Esqueletal, del Area Norte de la Región Metropolitana. Rev Dental Chile. 2001;92(3):15-9.
6. Hassan AH. Cephalometric characteristics of Class II division 1 malocclusion in a Saudi population living in the western region. Saudi Dental J 2011;23(1):23-7.
7.Rosenblum RE. Class II malocclusion: mandibular retrusion or maxillary protrusion? Angle Orthod 1995;65(1):49-62.
8. Craig CE. The skeletal patterns characteristic of Class I and Class II, Division I malocclusions in norma lateralis. Angle Orthod 1951;21(1):44-56.
9. Freitas MRd, Santos MACd, Freitas KMSd, Janson G, Freitas DSd, Henriques JFC. Cephalometric characterization of skeletal Class II, division 1 malocclusion in white Brazilian subjects. J Appl Oral Sci. 2005;13(2):198-203.
10. Pancherz H, Zieber K, Hoyer B. Cephalometric characteristics of Class II division 1 and Class II division 2 malocclusions: a comparative study in children. Angle Orthod 1997;67(2):111- 20.
11. Jacob HB, Buschang PH. Mandibular growth comparisons of Class I and Class II division 1 skeletofacial patterns. Angle Orthod 2014;84(5):755-61.
12. Soh J, Sandham A, Chan YH. Occlusal status in Asian male adults: prevalence and ethnic variation. Angle Orthod 2005;75(5):814-20.
13. Burgersdijk R, Truin GJ, Frankenmolen F, Kalsbeek H, van’t Hot M, Mulder J. Malocclusion and orthodontic treatment need of 15–74-year-old Dutch adults.Community Dent Oral Epidemiol 1991;19(2):64-7.
14. Tang EL. Occlusal features of Chinese adults in Hong Kong. Aust Orthod J 1994;13(3):159.
15. Ardani IGAW, Sanjaya ML, Sjamsudin J. Cephalometric characteristic of skeletal class II malocclusion in Javanese population at Universitas Airlangga Dental Hospital. Contemp Clin Dent 2018;9(Suppl 2):S342.
16. Burgos D. Prevalencia de maloclusiones en niños y adolescentes de 6 a 15 años en Frutillar, Chile. Int J Odontostomat 2014;8(1):13-9.
17. Aguirre Cortez P. Frecuencia de clases esqueletales segun el analisis de Steiner en pacientes entre 15 y 25 anos de edad del Programa de Especialización en Ortodoncia y Ortopedia Dentofacial de la Universidad de Talca entre los anos 2005-2009: Universidad de Talca (Chile). Tesis de grado. Escuela de Odontologia. Facultad de Ciencias de la Salud, Universidad de Talca, 2011.
18. Iturriaga R, Whittle M. Analysis of 1000 cases of dentomaxillaty anomalies. Rev Dent Chile. 1990;81(3):116-23.
19. Baccetti T, Stahl F, McNamara Jr JA. Dentofacial growth changes in subjects with untreated Class II malocclusion from late puberty through young adulthood. Am J Orthod Dentofacial Orthop 2009;135(2):148-54.
20. Sidlauskas A, Svalkauskiene V, Sidlauskas M. Assessment of skeletal and dental pattern of Class II division 1 malocclusion with relevance to clinical practice. Stomatologija. 2006;8(1):3-8.
21. McNamara JA. Components of Class II malocclusion in children 8–10 years of age. Angle Orthodon 1981;51(3):177-202.
22. Mizoguchi I, Toriya N, Nakao Y. Growth of the mandible and biological characteristics of the mandibular condylar cartilage. Japanese Dental Sci Rev. 2013;49(4):139-50. ´
23. Rothstein T, Yoon-Tarlie C. Dental and facial skeletal characteristics and growth of males and females with Class II, Division 1 malocclusion between the ages of 10 and 14 (revisited)—Part I: Characteristics of size, form, and position.Am J Orthod Dentofacial Orthop 2000;117(3):320-32.
24. Sharma BP, Xin C. Comparative cephalometric analysis of angle class II division 1 malocclusion between Chinese male and female subjects. Orthodont J Nepal. 2014;4(2):21-3.
25. Lacerda RHW, Silva AWC, Ramos TB. Assessment of upper airways measurements in patients with mandibular skeletal Class II malocclusion. Dental Press J Orthod 2015;20(5):86- 93.
26. Kannan A, Sathyanarayana HP, Padmanabhan S. Effect of functional appliances on the airway dimensions in patients with skeletal class II malocclusion: A systematic review. J Orthod Sci 2017;6(2):54.
27. Zaghi S, Holty J-EC, Certal V, Abdullatif J, Guilleminault C, Powell NB, Riley RW, Camacho M. Maxillomandibular advancement for treatment of obstructive sleep apnea: a meta-analysis. JAMA Otolaryngology–Head & Neck Surgery. 2016;142(1):58 66.
28. Rojo-Sanchis C, Almerich-Silla JM, Paredes-Gallardo V, Montiel-Company JM, Bellot-Arcís C. Impact of bimaxillary advancement surgery on the upper airway and on obstructive sleep apnea syndrome: A meta-analysis. Sci Rep 2018;8(1):1-8.
29. Ellis III E, McNamara Jr JA, Lawrence TM. Components of adult Class II open-bite malocclusion. J Oral Maxillofac Surg 1985;43(2):92-105.